A New Technology Provides a More Precise Measure of Pain

Columbia researcher uses quantitative sensory testing, or QST, for assessing the effectiveness of cannabis for therapeutic uses
How many times have you been asked to rate your pain on a scale of 1 to 10, from no pain to worst pain possible? It’s a pain measurement system commonly used, but it’s also recognized as being highly subjective and unhelpful, both for patients and physicians. After all, one person’s rating of 3 might be the same intensity of pain as another person’s rating of 5.
This inexact science poses problems for diagnosing and treating patients with pain. It also hampers researchers looking to develop new approaches and medications for pain, such as Caroline Arout, PhD, assistant professor of clinical neurobiology in Columbia’s Department of Psychiatry, who is studying—and attempting to quantify—the therapeutic effects of cannabinoids.
“With current technology, using the standard pain measurement system makes little sense, particularly when it comes to pain research,” Arout says.
Data for research and clinical use
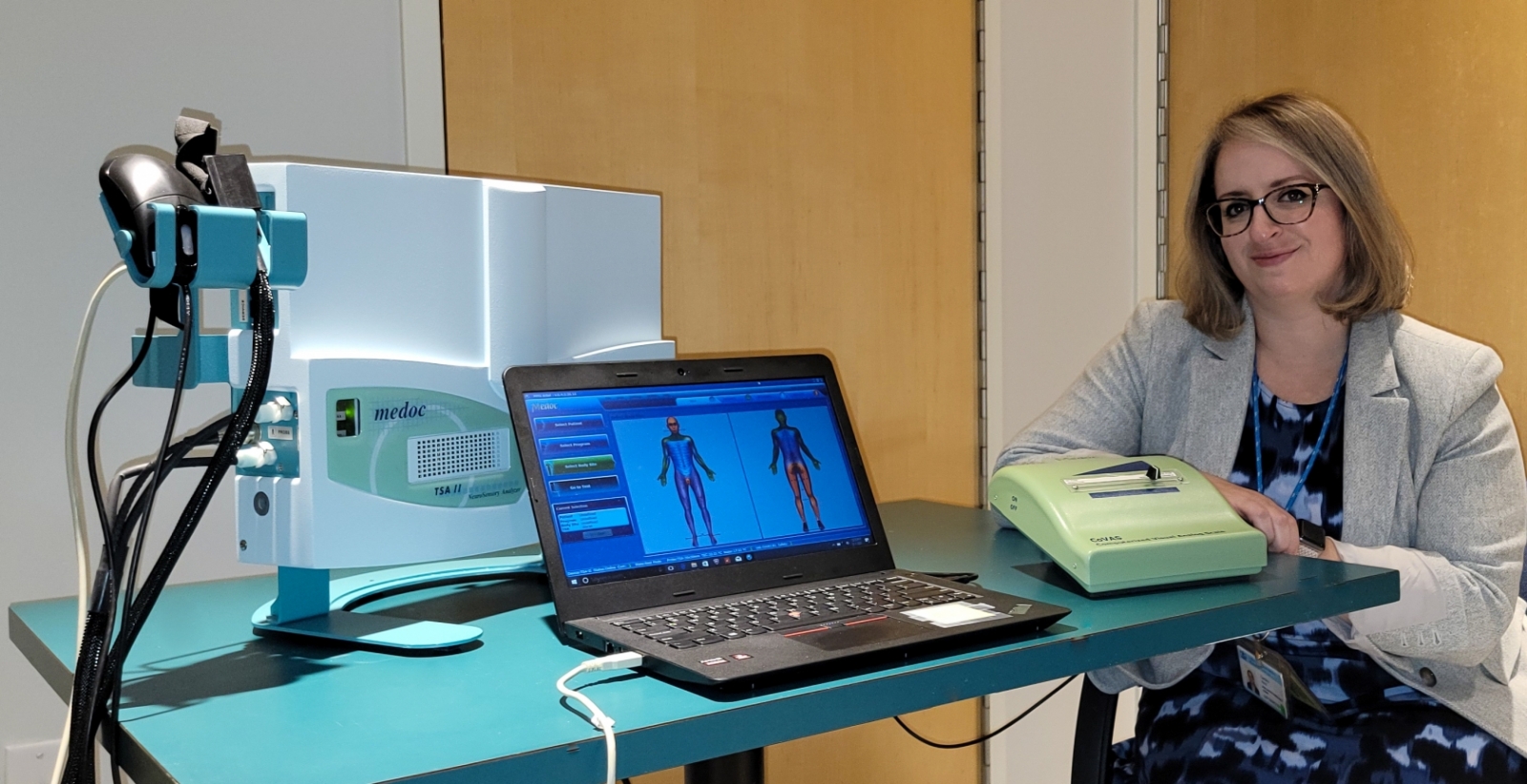
Instead, Arout is using a technological methodology known as quantitative sensory testing, or QST. It does a better job of measuring physical sensations scientifically and producing meaningful data for research and clinical use.
“The important difference between the two systems is that the numeric scale is based on perception and tolerance of pain, which varies from person to person, while QST offers a standardized experience,” Arout says.
Quantitative Sensory Testing has been used in only a few clinical settings, such as for measuring neuropathic pain. Now it’s receiving attention for possible applications with chronic pain, opioid use disorder, and more.
The technology measures nerve responses by using calibrated equipment to precisely apply different types of stimulation, including vibration and heat, cold, or pressure pain.
As a member of the New York State Psychiatric Institute’s (NYSPI) Cannabis Research Laboratory, directed by Margaret Haney, PhD, Professor of Neurobiology (in Psychiatry), Arout is using QST in two projects that are aiming to develop a model of cannabis-induced changes in pain perception over time. In their studies, the technology applies heat stimulation to measure effects of the two main cannabinoids, CBD (cannabidiol) and THC (delta-9-tetrahydrocannabinol).
Gauging the therapeutic effects of cannabis over time
Using the QST neurosensory analyzer, one study is using cannabis with high levels of CBD to examine its effects on the pain induced by the technology itself. The other, designed similarly, is investigating how repeated administration of high-THC cannabis affects pain over time.
For these projects—which are still seeking study participants—the QST equipment assesses temporal summation, an experimental correlate of central sensitization. When nerve cells become sensitized, Arout explains, that may be a marker of hyperalgesia (increased pain).
THC can relieve acute pain within 15 minutes, but many people use cannabis daily for chronic pain. “We don’t know how the effectiveness of cannabis for pain management changes over time with regular use, Arout says. QST will help the researchers answer that question.
In the studies, participants receive several pulses of heat. As the intensity of each pulse changes, they control a lever to indicate their pain perception on a scale of zero to 100. That’s still subjective, but it uses an exact stimulus over a precise period, so the researchers can quantify how participants are perceiving the pain.
Could QST help fight opioid addiction?
QST will not change pain perception, but it has been shown to be predictive for perioperative pain. Arout thinks it may prove to have applications in patients with opioid use disorder.
With more people looking to replace opioid pain medicines with a less addictive but still effective analgesic, such as cannabis, research is needed to understand the best ways to manage treatment. Through QST, the NYSPI studies aim to gauge if withdrawal from cannabinoids creates increased pain sensitivity, as withdrawal from opioids does.
“If people are starting to transition into using cannabis for pain,” Arout says, “we need to find those characteristics before we walk down that problematic road.”
Data from QST could be predictive for identifying patients at higher risk for developing opioid use disorder due to higher pain sensitivity and greater likelihood of using drugs to quell that pain. It also may have potential for predicting drug use outcomes.
Arout would like to see QST eventually used as a clinical biomarker as well as a research tool. She wants to explore whether people who show more pain sensitivity on QST measurements have correlative scores on scales of distress tolerance and pain catastrophizing, a behavioral inclination to magnify or repetitively think about anticipated pain.
“I would love to move this into a clinical pain population,” Arout says, “to use QST to understand how we can better address pain in different pain populations and how medications impact their pain perception.”
“The damage is done in terms of the opioid crisis,” she adds. “But how can we use QST to avoid that happening again?”
– Robin Warshaw
Dr. Arout’s studies are actively recruiting research participants. Her studies require a 16-day inpatient stay at the New York State Psychiatric Institute, where participants will smoke marijuana and undergo experimental pain, mood, and other assessments. Participants must be 18-60 years old and use marijuana. Please contact the laboratory at 646-774-7777 or e-mail Dr. Arout at Caroline.Arout@nyspi.columbia.edu for more information.